
bswift by the numbers
bswift invests in people and technology to create better experiences for all of those we serve.
View our mission
lives covered and experiences enhanced with bswift

Customer Service Transformation Award

Technology Excellence Award for Best Advance in Benefits Administration and AI-Human Collaboration

of clients retained due to our dedication to innovation and service
Clients that trust in bswift
“A few words to describe bswift technology: Flexible and user-friendly. Their ability to customize solutions for our complex organization really made a difference. I’ve truly enjoyed the partnership.”
-VP of Health and Welfare, Omnicom Group
bswift Benefits Administration Platform
Built for Complexity. Simplified for Scale.
Our AI-native benefits platform offers two configuration paths: Simplify for faster, pre-defined implementation. And Unlimited for fully customizable implementation when sprawling complexity calls for maximum control.
Available exclusively through
brokers & Channel Partners
bswift Simplify
Give growing groups a benefits upgrade.
Delivers the trusted bswift experience to employers whose complexity outgrows basic SMB platforms. Offers added control and automation without navigating full enterprise implementation.

Available to complex
employers & Channel Partners
bswift Unlimited
Turn complexity into calm.
Handles any workforce, anywhere with deep configurability and hundreds of integrations, so complexity never slows you down. Offers maximum flexibility and complete control.

Complete Benefits Administration
AI-native technology, hands-on service, and decades of expertise all working together to elevate every part of your benefits experience.

COBRA, Billing & Compliance Services
Reduce risk and take the regulatory workload off your plate.
We handle dependent verification, COBRA, retirement, and payroll reconciliation—combining AI precision with human expertise, so your team can stay focused while reducing risk.
Employee Engagement & Activation
Reduce confusion and drive year-round behavior change.
Boost participation with custom communications, while AI-guided experiences drive enrollment. From there, Evive powers utilization with personalized, data-driven nudges and year-round campaigns.

Employee Service & Support
Resolve issues fast with self-service plus expert human care.
Employees get instant answers through Emma™ Chat and IVR, while our Service Center provides expert, empathetic support for more complex moments. It’s how we keep enrollment season calm—and surprisingly quiet.
Connect with our team.
Get in touchTrusted by 300+ Enterprises
Beyond the RFP Checklist: Why Clients Choose bswift
Deep API Connectivity & Partner Integrations
Tap into 550+ pre-built and Partner integrations, including APIs with Workday, ADP, UKG and more.

Culture of Service Excellence
Your team's happiness is our #1 priority. We operate as an extension of your team and do whatever it takes to achieve your goals.
Emma Intelligence AI-Native Innovation
From chat to instant HR insights to unmatched decision support, native-AI technologies are changing the way you experience benefits.
Strategic Cost Optimization
Control benefits spend with precision. From eligibility validation to AI-powered insights, bswift gives you the levers to reduce waste, guide smarter decisions, and optimize plan design.
Connect with our team.
Get in touchFrequently Asked Questions

What is bswift?
bswift is a native-AI benefits administration platform that helps employers manage enrollment, eligibility, and compliance. The platform serves both large enterprises and small to midsize businesses through two configuration and implementation paths. The experience is enhanced by Emma™ Intelligence for automated employee support and more confident benefits decisions.
Who uses bswift?
bswift serves 300+ enterprise clients and over 16 million employees, including complex organizations with multi-location teams, unions, and variable workforces. The platform also supports brokers and Channel Partners service serving businesses of all sizes.
What services does bswift provide beyond benefits technology?
In addition to its benefits administration platform, bswift provides COBRA administration, billing and compliance services, employee engagement programs, and a 24/7 service center. These services help employers manage regulatory complexity while supporting employees throughout the year.
What is Emma Intelligence?
Emma™ Intelligence is bswift’s native AI layer embedded across the bswift ecosystem to make benefits simpler, smarter, and more human—reducing friction for employees, admins, and service teams. It uses benefits materials, plan configuration, eligibility logic, and operational context to guide decisions, accelerate answers, catch issues earlier, and turn data into direction.
What does native AI mean in Emma Intelligence?
Native AI means Emma™ Intelligence is built directly into the bswift platform and workflows—not added on as a separate chatbot or bolt-on tool. Because it runs on your real benefits configuration and content, it delivers plan-specific answers and automation that match what’s actually true for each employer and employee.
What is Evive and how does it work?
Evive™ is a capability built in to the bswift benefits platform that powers year-round personalized engagement. It uses eligibility data, enrollment history, and claims-aware insights to deliver targeted nudges and campaigns that encourage better benefits utilization. Evive helps sustain engagement beyond enrollment season and supports measurable savings through smarter usage patterns.
Can benefits administration platforms help reduce benefits costs?
Yes, benefits administration platforms can reduce costs by improving plan selection, preventing eligibility errors, and encouraging smarter healthcare spending. AI-driven guidance and data insights also help employers identify opportunities to optimize plan design and reduce unnecessary spend.
What’s the difference between bswift Unlimited and bswift Simplify?
bswift Unlimited gives larger, more complex organizations a fully customizable implementation path, offering maximum control to handle any global workforce. bswift Simplify® offers brokers and Channel Partners a faster, pre-defined implementation path to help growing groups move to an enterprise-grade experience without navigating full enterprise implementation.
Does bswift integrate with HR and payroll systems?
Yes, bswift integrates with leading HRIS and payroll platforms such as Workday, ADP, and UKG, along with hundreds of other partners through APIs and pre-built integrations. These connections allow employee data, eligibility rules, and payroll deductions to flow automatically between systems.
Does bswift handle COBRA administration?
Yes, bswift provides complete COBRA administration including initial notices, qualifying event processing, premium billing, election forms, and coverage terminations. Additional compliance services include dependent verification, payroll reconciliation, and ACA reporting.
What types of employers use bswift?
bswift supports organizations ranging from growing mid-market employers to large global enterprises with complex workforces. The platform is designed to scale across multiple locations, eligibility structures, plan types, and integrations.
What services does bswift offer beyond the platform?
bswift offers COBRA and compliance administration, dependent verification, payroll reconciliation, a 24/7 Employee Service Center, custom creative and communications, and Evive for systematic, data-driven employee engagement.
How do employees get benefits support with bswift?
Employees access bswift’s 24/7 Service Center, staffed by trained specialists augmented with native-AI Emma™ Agent Assistant, which delivers instant, accurate answers through phone, chat, and email—reducing HR burden and achieving 96% satisfaction rates.
How is bswift different from other benefits administration platforms?
bswift differentiates through purpose-built enterprise complexity, handling 550+ pre-built integrations, white-glove service with dedicated Client Success Managers, in-house engagement expertise, and 98% client retention—versus platform-only competitors focused on simple scenarios.
Is bswift reliable?
bswift maintains 98% client retention, 96% Service Center satisfaction, supports 16 million lives across 300+ enterprise clients, and has received recognition for innovation from Brandon Hall Group for the past 5 years—demonstrating consistent platform reliability and service quality.
What's New

Product Updates March 2026
Enhanced personalization from Evive connects employees to the right benefits at the right time, improving outcomes and reducing costs. Emma Chat and new mobile updates make it easier for employees to get answers and take action.

The Enduring Power of Personalization in Benefits
Personalization delivered at scale can support proactive resolution—but its real power lies in shaping smarter decisions, helping people access care earlier, and reducing avoidable healthcare spend.

The Real Cost of Running Benefits Through Your HRIS
HRIS platforms often position benefits administration as an easy add-on: one system, one contract, one vendor.

GLP-1s, TrumpRx, and the PBM Transparency Push: A 2026 Primer for HR Leaders
Learn how holistic health trends in employee wellbeing programs like value-based care, whole person care, mental health.
bswift Beacon Ep. 07: How HR Can Finally Play Offense on Healthcare Cost Spikes with Ted Bloomberg
bswift CEO Ted Bloomberg joins Denise and Joel to unpack the reality of 2026’s healthcare cost spike—and why the old playbook just doesn't cut it anymore.

Product Updates January 2026
New personalization enhancements help employees stay on track with a tailored benefits checklist and more dynamic, data-driven engagement powered by Evive. Employers gain deeper insight into employee preferences, while new reporting tools surface issues quickly and reduce risk.

The High Cost of All-in-One HRIS Benefits: Why Consolidation Costs More Than It Saves
There’s a reason “penny wise and pound foolish” has survived centuries of business wisdom.

Empowering HR to Navigate Open Enrollment 2025 with Confidence
Stress-free annual enrollment starts with bswift. Explore our infographic for HR tech, stellar service, and employee satisfaction at light speed!

Hospital Benefits Administration: Simplify Healthcare Workforce Benefits and Contain Costs
Learn how holistic health trends in employee wellbeing programs like value-based care, whole person care, mental health.

Product Updates December 2025
Enhancements to Emma EnrollPro deliver more precise, personalized decision support, helping employees make more confident benefit choices aligned with your strategy. New dashboards and improved integrations provide faster insights and stronger data connectivity.

Total Rewards Communication: The Retention Strategy HR Keeps Overlooking
Annual enrollment communication doesn’t have to be chaotic. Build trust with employees and simplify decision-making with actionable HR strategies.

bswift Beacon Ep. 06: Leading HR & Culture During Open Enrollment with Natalie Atwood
bswift CPO Natalie Atwood shares strategic HR leadership advice for open enrollment, including building relationship capital, using feedback, and moving HR from administrative to strategic.

Leveraging AI to make every experience simpler, smarter, and more human
Annual enrollment communication doesn’t have to be chaotic. Build trust with employees and simplify decision-making with actionable HR strategies.

Thriving Through Open Enrollment: Lessons from bswift’s Chief People Officer
It’s open enrollment season — HR’s annual enrollment Super Bowl, where strategy meets sheer endurance.

Is Your Benefits Software Helping or Hurting? The Truth about HRIS vs. Benefits Platforms
Annual enrollment communication doesn’t have to be chaotic. Build trust with employees and simplify decision-making with actionable HR strategies.

Mindful AI: Our Philosophy for Responsible AI in Benefits
AI is everywhere in HR right now. Every conference, every panel, every software demo — it’s the headline act. And if you’re in charge of benefits, you’re already feeling the squeeze.

Product updates September 2025
New enhancements support compliance and efficiency with improved IRS contribution limit configuration and near real-time UKG Pro integration. Real-time enrollment confirmations and streamlined admin navigation create a faster, more connected experience for both employees and administrators.

Why Millennials and Gen Z Tune Out and How Personalized Employee Benefits Communication Changes Everything
Discover why Millennials and Gen Z ignore employee benefits and how HR leaders can boost engagement with personalization, AI, and smarter communication.
Beyond Checkboxes: Annual Enrollment Strategies That Engage and Deliver
Boost employee and benefits engagement with actionable strategies from this bswift SHRM webinar replay. Watch now and earn SHRM credit!
bswift Beacon Episode 05: Climbing the Annual Enrollment Mountain with Amit Jain
Joel and Denise are joined by Amit Jain, COO of bswift, to discuss the challenges of annual enrollment and how HR teams can navigate this busy season.

Legislative Update: What the One Big Beautiful Bill Act Means for Employers
Prepare for enrollment season with our open enrollment checklist! Discover tips, strategies, and a comprehensive checklist to streamline your planning and execution.

Benefits Administration Solution Buyer’s Guide for HR Teams
Download this HR Buyer’s Guide to benefits administration solutions. Learn how to compare vendors, evaluate features, and build a business case with real ROI.

How to Navigate (and Win) Open Enrollment Season
Prepare for enrollment season with our open enrollment checklist! Discover tips, strategies, and a comprehensive checklist to streamline your planning and execution.

How Annual Enrollment Communication Can Help HR Build Employee Trust
Annual enrollment communication doesn’t have to be chaotic. Build trust with employees and simplify decision-making with actionable HR strategies.
Product Updates July 2025
New enhancements expand Emma EnrollPro to deliver more holistic, personalized recommendations while improving admin efficiency with on-demand tools and built-in safeguards. Enhanced API integrations and automation streamline operations for brokers and partners.

bswift Beacon Episode 04: HR AI and Emma Intelligence in Focus with Vinita Pilani
Joel and Denise are back with bswift Beacon, this time joined by bswift’s Senior VP of Product Engineering, Vinita Pilani, to discuss the evolution of HR tech.
How bswift’s Service Center Is Redefining Employee Benefits Support
Hear how bswift's Service Center blends HR tech and empathy to transform employee benefits support—driving a 95% satisfaction rate.

Wellbeing, Rewired: Employee Benefits in 2025
Discover four strategies HR leaders can use rebuild clarity, foster connections, create meaningful growth opportunities and boost employee engagement.

Next Gen HR: Recapping Ben Admin’s Bright Future at bswift’s Idea Exchange 2025
Every once in a while, an event brings together the kind of energy, ideas, and people that not only spark change but drive it forward. That’s exactly what happened at bswift’s Idea Exchange (IX) 2025.
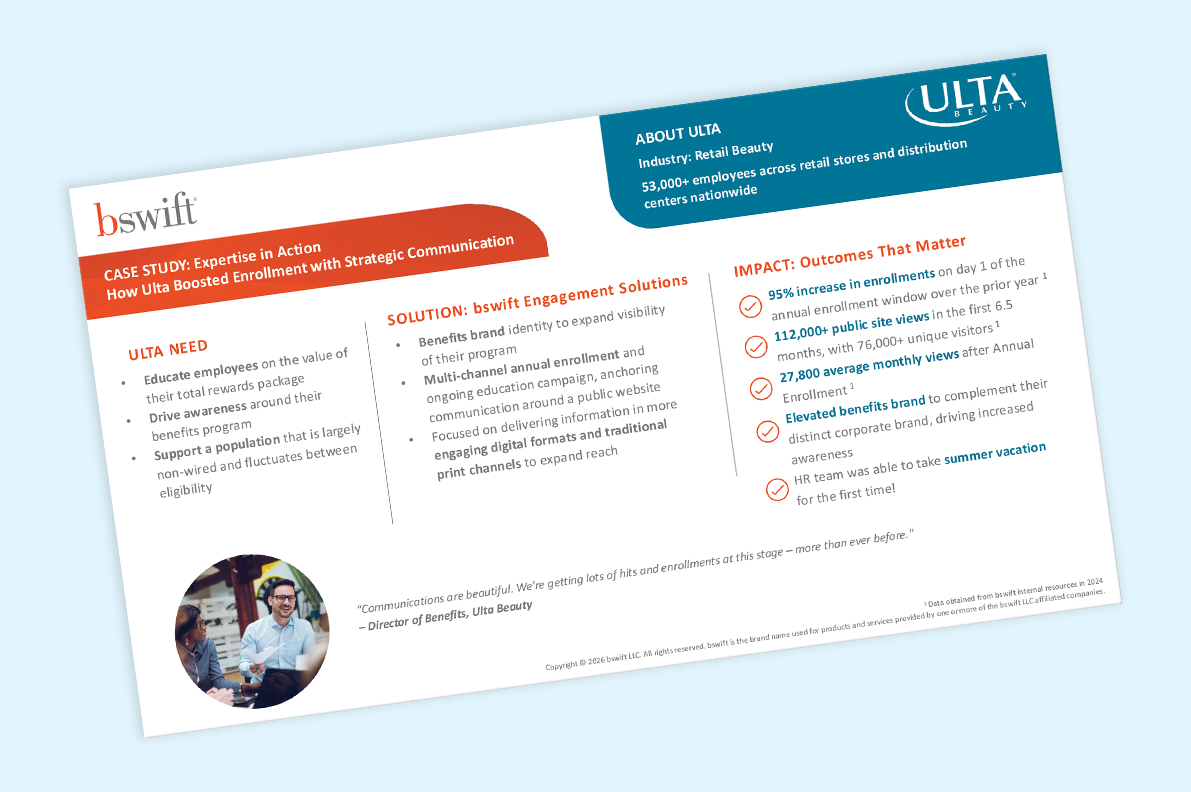
Benefits Engagement Strategy: Ulta’s Success Story
With 53,000+ employees across stores and distribution centers, Ulta needed a new approach to employee benefits communication—one that could reach a largely non-wired workforce.
bswift Beacon Episode 03: LIVE from Idea Exchange with Scott Millson on Leadership and Finding Your Frequency
Join hosts Denise and Joel for a special live episode of the bswift Beacon podcast, recorded at bswift’s Idea Exchange conference in Hollywood, FL.
Streamlining Success: Cabot Corporation’s Partnership with bswift
Hear how bswift’s responsive partnership and intuitive solutions simplify enrollment, payroll, and data management while delivering exceptional support and empowering HR.

How MMA Delivers Big Results with bswift’s Powerful Benefits Platform
Learn why MMA partners with bswift to streamline benefits management, improve HR operations, and enhance the employee experience.
Idea Exchange 2025: On-Demand General Sessions
Dive into some of the top sessions from Idea Exchange 2025—now available to watch anytime. Whether you're reimagining your benefits strategy, improving the employee experience, or navigating the future of HR, these expert-led presentations offer practical insights and actionable solutions to help you stay ahead.
Product Updates May 2025
New updates enhance the employee experience with real-time confirmations, personalized support, and more accessible tools across mobile and family portals. At the same time, AI-powered automation and expanded API capabilities help administrators streamline processes, reduce errors, and scale more efficiently.
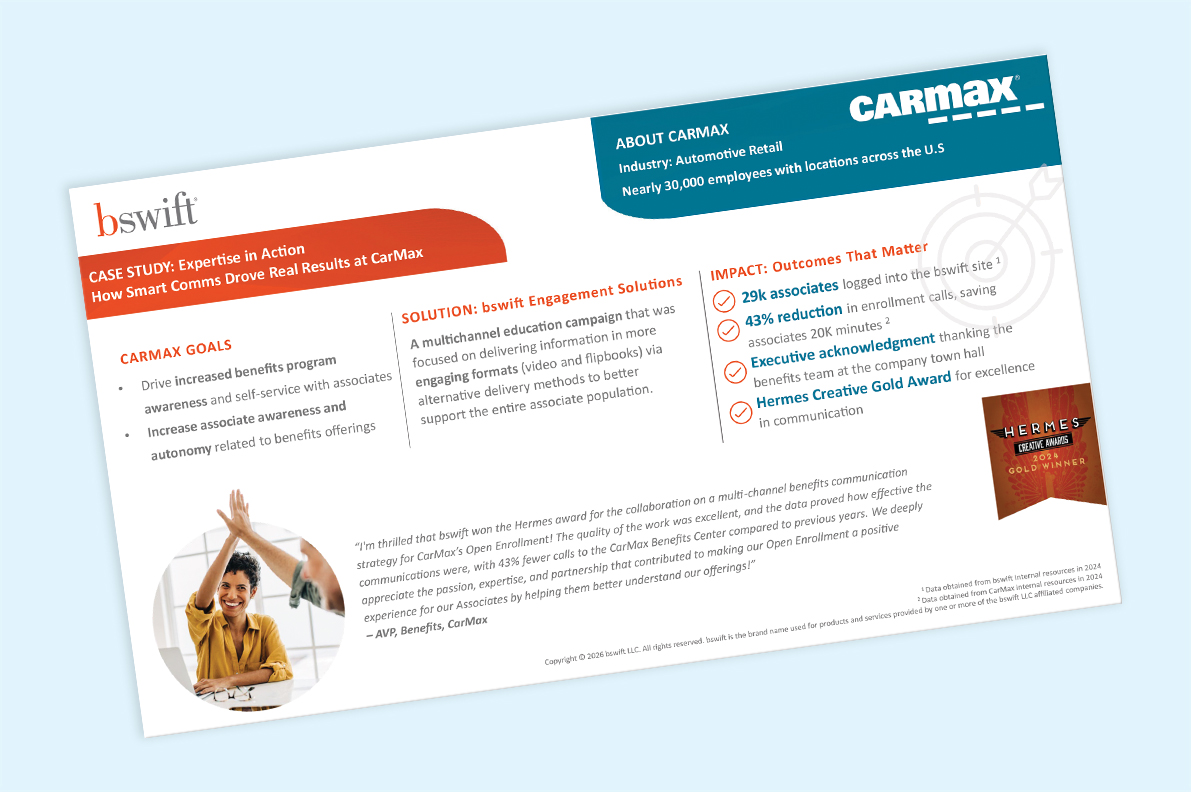
CarMax’s Success with Strategic Employee Benefits Communication

How RRD Simplified Employee Benefits Enrollment and Elevated Engagement
With a large, globally distributed workforce, RRD faced the challenge of transitioning employees to a new healthcare plan—without disrupting the enrollment experience. RRD and bswift partnered to deliver innovative solutions to streamline employee benefits enrollment and deliver positive results.
bswift Beacon Episode 02: The Future of Service Excellence with Eric Strom
Join hosts Denise and Joel for an insightful discussion with Senior Vice President of the bswift Service Center, Eric Strom, the driving force behind bswift’s Service Center transformation.
Enhancing Wellbeing with bswift’s Incentive Program
Struggling with low engagement with preventive health measures and rising healthcare costs? Large companies across North America are utilizing Evive™, bswift’s personalization engine and incentive-based program, to help.

4 Steps to Build a Business Case for Better HR Tech Investment
Whether it’s clunky manual tasks, confused employees, low engagement, or compliance risks, your current system is frustrating and feels like it’s holding you back.
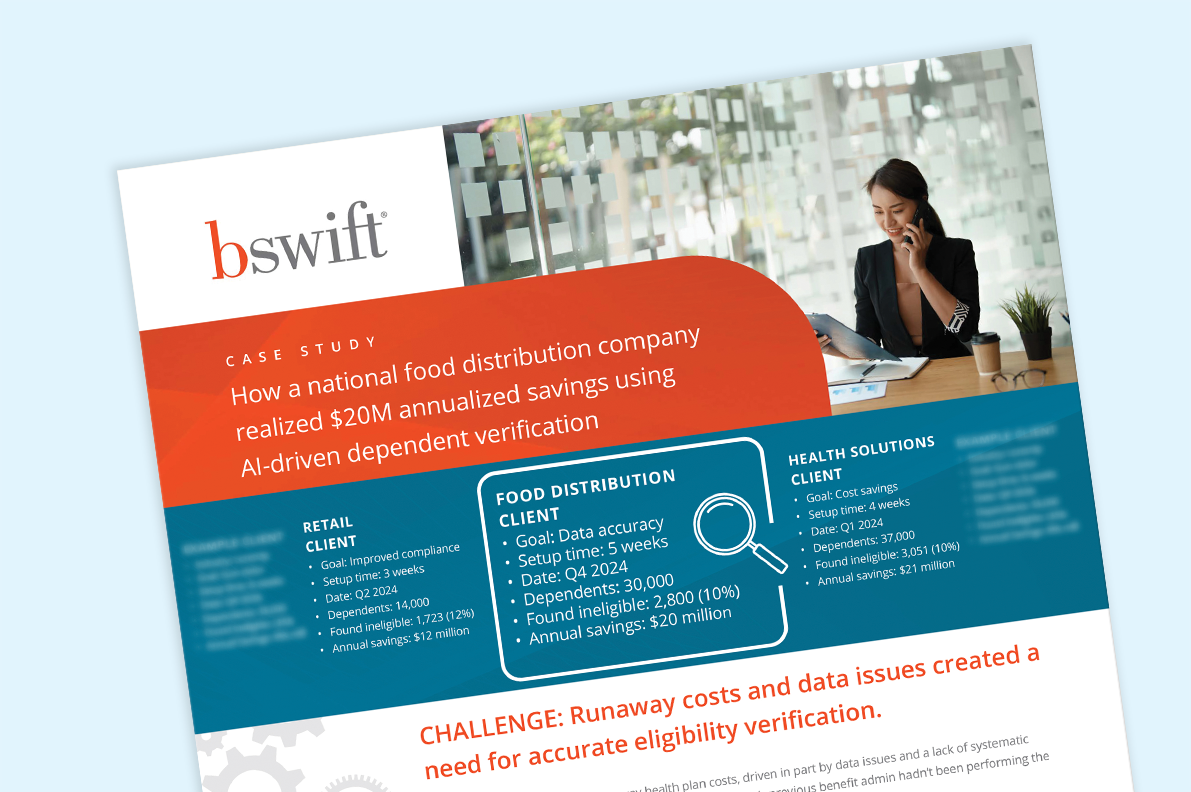
National Food Distributor Saves Millions with AI-Driven Dependent Verification
To help a client facing rising health plan costs due to data inaccuracies and inefficient verification processes, bswift deployed its AI-powered dependent verification audit in just two weeks.

SHRM Webinar Replay: Solving the Employee Engagement Crisis
Boost employee and benefits engagement with actionable strategies from this bswift SHRM webinar replay. Watch now and earn SHRM credit!
MaineHealth Boosts Voluntary Benefits Enrollment with Comprehensive Strategy
Discover how MaineHealth boosted voluntary benefits enrollment by updating carriers, enhancing plan designs, expanding communications, and using bswift’s Emma for personalized guidance.
bswift Beacon Episode 01: Cracking the Code on Employee Engagement with Alyssa Zeff
Join hosts Joel and Denise for the debut episode of bswift Beacon. Get insights from internal communications expert Alyssa Zeff.
Product Updates February 2025
New enhancements improve mobile access and engagement with easier login options and proactive billing reminders for employees. At the same time, expanded integrations, automation, and AI-powered tools help streamline operations, improve data accuracy, and increase efficiency for administrators and partners.

HR Trends That Will Define 2025: Rising Costs, Smarter Benefits Strategies
Discover the HR trends shaping 2025, from skyrocketing healthcare costs to smarter benefits strategies. Learn how to stay ahead and support your team.
Product Updates December 2024
Enhanced personalization, smarter Emma Chat, and improved mobile features make it easier for employees to engage with their benefits and make informed decisions. At the same time, updates to bswift Simplify help brokers and partners streamline renewals and reduce manual effort.

bswift Delivers a Stellar Annual Enrollment
Stress-free annual enrollment starts with bswift. Explore our infographic for HR tech, stellar service, and employee satisfaction at light speed!

The Rising Impact of Diabetes on Workplace Productivity and Employee Health
Support employee health and reduce costs with effective diabetes management programs that promote workplace wellness and enhance productivity.

Values in Action: How Company Culture Drives Business Success
Here's how strong company culture, driven by core values, improves employee engagement and business success. Learn how to strengthen culture.
The Winning Annual Enrollment Trifecta
Our annual enrollment infographic unlocks the power of effective communication, AI, and human expertise for a seamless benefits experience.

AI for Health Plan Administration: 3 Ways It’s Transforming Benefits Management

The Winning AE Trifecta: AI, Employee Comms and Human Connection
In this webcast, bswift will explore how HR can optimize annual enrollment (AE). They’ll cover marketing-inspired communication techniques, the role of AI in streamlining HR processes, and the importance of the human touch.

Conquer Annual Enrollment: 7 Steps to Scale Your HR Everest
Master annual enrollment with our checklist. From HR tech to communication planning, streamline your HR process and improve your employee benefits rollout.

Product Updates August 2024
Enhancements to Emma EnrollPro and Emma Chat, along with new mobile features, make it easier for employees to navigate benefits and make informed decisions. At the same time, expanded automation, AI-powered tools, and updates to bswift Simplify help streamline operations and improve efficiency.
bWise – Ep 30: Emma™ Asks the Experts: The Future of AI in Benefits Administration
Join hosts Don and Sharon as they explore the latest AI enhancements to bswift’s groundbreaking AI-powered platform intelligence, Emma.

4 Holistic Health Trends to Boost Employee Wellbeing and ROI
Learn how holistic health trends in employee wellbeing programs like value-based care, whole person care, mental health.

Flexible, Powerful, Trusted: bswift Redefines Benefits Admin
Hear why HR pros choose bswift for benefits administration. See why organizations of all sizes trust bswift to deliver efficiency, flexibility, and advanced functionality in benefits tech.

AI for HR: 4 Key Trends You Need to Know Now
Cut through the hype. From Mindful AI to people analytics, these 4 trends in AI for HR boost employee engagement and attract top talent.

Harnessing the Power of AI for HR
Unlock AI’s potential in HR with bswift: Automate tasks, enhance decision-making, and focus on strategic goals. Discover AI’s role in recruitment, onboarding, and more

bWise – Ep 29: Building the Future of HR with AI: A Chat with Jeff Kirk
Get practical insights for driving successful digital transformations across industries. Listen in as Jeff Kirk shares his 20+ years of experience and wisdom, with real-world examples of digitizing businesses

Employee Healthcare Cost Containment Strategies:
A Guide for HR
Rising healthcare costs got your HR team down? Discover 4 data-driven cost-containment strategies from bswift's IX to reduce healthcare spending & improve wellbeing.

Harnessing the Power of AI for HR – Make it Mindful
Leverage AI for HR with bswift's Mindful AI approach. See how AI enhances human expertise, recruiting, onboarding, engagement and compliance.

The Gold Standard in Employee Comms: bswift Engagement Solutions
bswift Engagement Solutions wins 2 Gold Hermes Awards for creative employee benefits communication. Learn more about our award-winning work!

Introducing the AI Supercharged Emma™: Your Employee Benefits Guide
Empower your employees with bswift's Emma, an AI-powered benefits assistant. Personalized recommendations, plan comparisons and more.
Simplify Benefits, Unlock HR’s Potential: bswift Has You Covered
Simplify benefits administration and empower HR with tools to streamline enrollment, optimize benefits use, and free HR for strategic work.

Solving the Employee Communication Puzzle: Tips for Better Engagement
Effective employee communication is crucial for HR. Learn best practices to improve benefits utilization and employee engagement.

bWise – Ep 27: Streamlining Benefits Admin: Real-World Wisdom from Industry Vet Maria Yao
The latest episode of the bwise Podcast is a masterclass in optimizing operations. Tune in for Maria’s straight-shooting advice and elevate your operational capabilities.
Flexible and User-Friendly: bswift Benefits Enrollment Solutions
Learn how bswift’s benefits administration platform streamlines HR’s work with flexible technology, seamless customization, and user-friendly tools to deliver benefits the way they’re meant to be.
Ditch the Stress: How bswift Makes Benefits Administration Easy
bswift’s innovative platform takes the hassle out of benefits administration. See how we empower HR with user-friendly tools to help deliver benefits.

bWise – Ep 26: Achieving Liftoff: Lana Hillebrand’s Journey From Astronaut Aspirations to HR Industry Leader
In this episode, hosts Don and Sharon sit down with HR and benefits administration leader Lana Hillebrand, who recently joined bswift’s advisory council.

Optimize Benefits Enrollment: HR Best Practices for the ‘So-Called’ Off-Season
Benefits enrollment best practices for HR. Improve employee communications strategies, analyze benefits utilization and enhance benefits portfolios.

bWise – Ep 25: Navigating the Future of Ben Admin: A Conversation With Scott Millson
On this episode, benefit administration insider Scott Millson shares his unique perspective on his over three decades in the employee benefits field.

American Heart Month: How to Support the Heart Health of Your Workforce
February is American Heart Month – the perfect time to focus on workplace wellness and heart health through personalized digital tools and connected capabilities.
Choosing Your Benefits with Ask Emma
Choosing Your Benefits with Ask Emma Video Transcript

The Future of HR: 4 Trends Reshaping Employee Benefits in 2024
Let's look at the future of HR, from AI and automation to cost containment, tailored well-being initiatives, and adapting to remote work.

bWise – Ep 24: Ice Baths to Client Service Excellence: A Conversation With bswift COO Amit Jain
Listen in as bswift Chief Operating Officer Amit Jain talks about his passion for client service, his unique approach to leadership, and his vision for the future of benefits administration technology.

Paycor Channel Partner Story
Learn how the expertise, seamless integration, and customer-focused approach of benefits admin platform bswift supports Paycor. Watch Video.

NFP Channel Partner Story

Bolton Channel Partner Story
Bolton partners with bswift for an intuitive, user-friendly benefits platform and exceptional support. Watch video now.

How to Improve Employee Benefits Engagement
Boost employee benefits engagement with proven HR strategies like clear communication, feedback loops, and AI chatbots to empower employees

bWise – Ep 23: Shaping Culture and Service: A People-First Approach to HR with bswift’s Natalie Atwood
bswift’s Chief People Officer Natalie Atwood talks with bWise hosts Don and Sharon about her passion for putting people first.

bswift Elevate™: Empowering Holistic Employee Wellbeing, Anywhere and Anytime
bswift Elevate is reimagining the employee well-being journey and simplifying the employee experience with hyper-personalized messaging to drive deeper engagement in employer wellbeing programs.

The bswift Service Center Commitment Video
Benefits can be difficult to understand. Watch this video to see how bswift's Service Center makes it simpler for employees.

Want Engaged Employees? Show Full Value with Total Compensation Statements
A smart way to boost employee engagement is to create a total compensation statement that details the value of their salary, benefits and other rewards.
The bswift Service Center Commitment
At bswift, we supplement our innovative and flexible HR tech with a strong commitment to service excellence.

Toyoda Gosei Customer Story
Hear how bswift’s benefits tech stands out for its robust functionality, flexibility and dependability in managing complex benefits for a diverse workforce.

GXO Customer Story
See how bswift’s flexible solutions and services helped GXO quadruple their benefits enrollment rate. Watch Video here.
bswift Mobile App: Empower Your Employees
The bswift Mobile App offers your employees seamless access to their benefits. Download the app now via the App Store or Google Play Store.

Omnicom Group Customer Story
See how bswift’s flexible solutions and services helped Omnicom navigate their complex benefits administration needs. Watch now!

Ace Annual Enrollment: 4 Solutions to Common HR Challenges
Make annual enrollment frictionless and empowering, These tips will help you optimize the employee experience and drive talent retention.

Unlocking the Power of Employee Benefits
Discover the hidden keys unlocking the full value of your benefits program for your employees and your organization. Watch it now!
Prioritizing Employee Wellbeing for Business Success
Explore the core connection between employee benefits, employee wellbeing, and business success. Get a roadmap for reviewing your organization's current offerings to ensure they're relevant, accessible and effectively supporting workforce health and productivity.

Insights and Highlights: A Recap of bswift’s Idea Exchange 2023 Conference
bswift's Idea Exchange 2023 Conference brings you insights on employee benefits engagement and benefits administration. Access session videos and more. Perfect for any HR professional looking to stay up-to-date.

bWise – Ep 20: Digital Transformation: HR and Employee Engagement, With NFP’s Mark Rieder
In this episode, we’ll explore how digital transformation can improve the employee experience, boost customer satisfaction, increase productivity, and drive greater profitability for the company.
Fueling Outcomes: bswift’s Innovation Strategy and Latest Enhancements
Watch bswift's latest video to get up to date on bswift's latest innovation strategy and enhancements. Watch video now.

bWise – Ep 22: Driving Operational Excellence at bswift With Adam Hostetter
Get an insider’s look at how bswift’s Head of Operational Excellence, Adam Hostetter, is driving major improvements. Learn how his team is enhancing service delivery, upgrading technology, and aligning workstreams to accelerate growth.

Hire Emma: bswift’s AI HR Assistant That Pays for Herself
Meet Emma, the AI HR assistant who resolves benefits questions, provides enrollment guidance, and improves the employee experience.

bWise – Ep 21: bswift’s Bright Future, Mission, and Passion, With bswift CEO Ted Bloomberg
In this episode, you’ll learn more about bswift’s leadership, what fuels our passion for our clients and partners, and our commitment to deliver excellent technology and service to all those we serve.

Here’s How to Create An Engaging Employee Benefits Communication Strategy
Great employee benefits communication is crucial for employee satisfaction. Get tips for effective benefits communications that engage all stakeholders, using a multi-channel approach, incorporating empathy, focusing on timing, highlighting total rewards, and broadening the conversation on employee wellbeing.

Unlocking the Power of Employee Benefits
Employee benefits are key to attracting, engaging and retaining top talent. Read this infographic to learn more on the underutilization gap

The Power of Effective Employee Benefits Utilization: Tips to Boost Benefits Engagement and Retention
Improve retention, engagement, wellbeing and productivity with an effective employee benefits utilization strategy. Boost benefits engagement with these tips.

Maximizing Employee Benefits Utilization: Challenges and Solutions
Improve engagement and retention with effective employee benefits utilization. Learn common challenges, solutions, and the importance of prioritizing employee wellbeing.

Forrester Research Reveals the High Cost of Low Employee Benefits Engagement (And What You Can Do About It)
Discover how HR pros can improve employee benefits engagement with insights from Forrester Research. Boost morale, productivity and retention, and cut healthcare costs. See the survey results and actionable strategies now.

The Top 5 Employee Benefits to Boost Satisfaction, Retention and Recruitment
Learn which employee benefits matter most to employees, and how these top employee benefits boost satisfaction, retention, and recruitment. A must-read for HR professionals.

How to Use AI to Improve HR: bswift Experts Answer CHROs’ Most Pressing Questions
bswift experts answer CHROs' questions about using AI to improve HR. Learn how to avoid pitfalls, partner with CTOs, and create a better employee experience.
How to Successfully Implement AI in HR: The CTO and CHRO Partnership
Let's look at the benefits and the risks of AI in HR. From data privacy to legal liability, CHROs and CTOs can partner to safely implement AI for business.

Boost Benefits Utilization with a Great Employee Benefits Communication Plan
Unlock the full potential of your employee benefits communication. Benefits U helps you save time and effort and boost employee engagement.
Webinar: Ask the Experts – How to Make AI an Essential Workforce Tool
Artificial intelligence is set to revolutionize the way we manage workforces. Watch our webinar to take your AI knowledge to the next level
ACA Management Suite
Introducing ACA Management Suite, offering a suite of management solutions to help employers navigate the new world of healthcare and benefits

Cut Costs, Not Benefits: Establish a Culture of Health in Your Workplace
Learn how to reduce healthcare costs and improve employee satisfaction with a culture of health in the workplace. Follow these 6 easy steps.

Celebrating Black History Month with Benefits Equity
How you can make the most of this celebration by incorporating employee benefits into your diversity, equity, and inclusion strategy.
6 Great Questions To Help You Measure Annual Enrollment Success
With the dust settling on annual enrollment, it's time to look back and learn. Here are a few simple questions you and your HR team can ask.

The Top 5 HR Trends of 2023: Leveraging Tech to Put the ‘Human’ Back in HR
In 2023, technology will continue to play a major role in how we adapt. Here are the top five HR trends we’re watching in 2023.
The 3 E’s and bswift’s New Homepage Experience
Your benefits homepage is the launching point for all things benefits, check out this infographic to see how bswift's new home page experience makes the 3 E's stress free.

bswift Dashboard and Reporting
The bswift Dashboard and Reporting tool provides easy access to the robust data you need in customizable reports, all in one location.

Solving the Great Resignation: The role of employee-centric benefits, tech & culture
Struggling to navigate the Great Resignation? Here are a few ways to improve and develop a more employee-centric-culture.

We are bswift
We are bswift video transcript: From innovation and data security to compassion and care, hear from our people about what makes us bswift.

Brown & Brown Channel Partner Story
A bswift Channel Partner Story, on why Brown & Brown Insurance partnered with bswift
DirectPath Channel Partner Story
A reliable partner for DirectPath, "with bswift, we know that when they say they can do something, they can do it.”

HealthPass Channel Partner Story
Explore why Channel Partner, HealthPass, partnered with bswift to enter the competitive healthcare benefits workspace.

Partner Customer Story
Watch to see firsthand why enterprises across the country choose our bswift platform to transform benefits administration.
Sony Corporation of America Customer Story
Read how Sony gained efficiency with bswift.
ICUBA Customer Story
Watch customer story now

Texas Roadhouse Customer Story
Watch customer story now.

EnPro Industries Customer Story
Learn how EnPro Industries boosted enrollment with bswift.
Holcim US Customer Story
See firsthand how our platform transforms benefits administration.
